
The science behind ankylosing spondylitis: Current mechanisms and emerging findings
Introduction
This review aims to explore the mechanisms of ankylosing spondylitis to suggest areas of research for potential cures. Ankylosing spondylitis is an autoimmune disease that causes excessive inflammation of the joints, most commonly affecting the spine. This disease is often accompanied by abnormal bone growth in joint cavities and spine fusion, causing permanent damage if not diagnosed and treated promptly. Pain from inflammation and bone spurs can be debilitating, sometimes keeping patients bedridden.
Scientists have not yet determined the root cause of ankylosing spondylitis, resulting in no known cure. An estimated 3.2 million American adults are currently living with spondyloarthritis-associated diseases, making it more common than rheumatoid arthritis, multiple sclerosis, and amyotrophic lateral sclerosis (ALS) combined.1 Despite its prevalence, AS remains under-investigated compared to similarly debilitating diseases in terms of available literature and research. The Spondylitis Association of America keeps a page updated with research breakthroughs, but the most recent paper was published almost ten years ago in 2015. Even without a known cause, treatments are available for mediating the symptoms of ankylosing spondylitis in the form of anti-inflammatory and immunosuppressive drugs such as inhibitors of TNF-α, IL-17, or JAK proteins. These treatments are often insufficient, as many patients either do not respond properly or their immune systems eventually adapt, rendering the drugs ineffective.2 Furthermore, immunosuppressive drugs increase patients' susceptibility to opportunistic infections, leading to a lower quality of life due to more frequent illnesses.
In 1973, AS was found to be associated with the HLA-B27 gene. Since then, there have been few breakthroughs on the causes of ankylosing spondylitis beyond this association, which isn’t even a perfect correlation. Ankylosing spondylitis can be diagnosed without the HLA-B27 marker, and patients can be HLA-B27 positive without developing associated diseases. Most White Americans with AS are HLA-B27 positive, but only 50% of Black Americans with AS are HLA-B27 positive.1 Other genes that have been associated with AS in the absence of HLA-B27 are ERAP-1, IL1A, and IL23R.3 Conversely, only 5% of people who are HLA-B27 positive will develop AS.4 Another unexplained oddity about ankylosing spondylitis is its predisposition in males, whereas all other known autoimmune diseases are more commonly found in females.5 This research suggests there is more to developing AS than expressing the HLA-B27 gene, but no further conclusions have been made regarding other causes.

Most medical researchers will not receive grant funding for research proposals if they do not have plausible likelihoods for success or feasibility, which means that determining the cause of ankylosing spondylitis is key to initiating research on finding a cure.
Methods
This review was done by a literary search of online databases. The databases used were the NIH Library, PubMed, Frontiers, and the Wiley Online Library. The search terms included were Spondyloarthritis, Lupus, Car T Cell Therapy, Causes, Ankylosing Spondylitis, Lupus, Gene Therapy, and HLA-B27. Publications older than five years ago (2019) were excluded from the results section to ensure that all research was current. These excluded publications were only used to provide background and introductory information. Results were further narrowed by evaluating abstracts and methods to determine if the research was focused on finding the cause of AS rather than the treatment of symptoms.
Background
The HLA-B27 gene codes for the HLA-B27 protein found on the surface of leukocytes. HLA stands for Human Leukocyte Antigen, which is the human-specific Major Histocompatibility Complex (MHC). MHCs are special receptors found on almost every cell type in the body and are vital for the function of the immune system by displaying antigens to alert T cells. During an infection, pieces of pathogens (disease-causing agents) are processed and attached to MHCs, such as HLA-B27, on somatic cells that have been infected. HLA-B27 then holds onto the pathogen fragment so that nearby cytotoxic T cells can bind the HLA-B27 and discover the pathogen, raising the alarm and beginning the immune response.
The more variability there is in the immune components, the higher the chances of discovering and destroying different pathogens. Each person has different HLA receptors that can be expressed, due to genetics and the environment. The gene for HLA-B27 is passed down genetically, and it is estimated that about 6% of the population has it.3 HLA-B27 is one of many types of MHC found in our cells, although HLA-B27 receptors are most commonly found in the epithelial cells of the joints, eye, digestive tract, and heart, which is where the worst symptoms of AS develop.
Historically, symptoms for autoimmune diseases such as AS have been treated with drugs that suppress Tumor Necrosis Factor (TNF-α), Interleukin 17 (IL-17), or Janus Kinase (JAK). TNF-α is a cytokine, an inflammatory chemical messenger, that is released by immune cells to disrupt the tight junctions between epithelial cells, thus increasing blood vessel permeability and causing the inflammation that precedes joint pain. IL-17 is another cytokine released by T-helper 17 cells (Th17), a subtype of helper T cell that specializes in recruiting phagocytic immune cells to destroy bacteria. Finally, JAKs are intramembrane cellular receptors triggered by cytokines like IL-17 to activate transcription factors to produce more cytokines. Most immunosuppressants target these three proteins as a blanket solution to decrease inflammation, a common symptom in many autoimmune disorders.
Results
Two Leading Hypotheses
Two leading hypotheses on the causes of HLA-B27-mediated inflammation are the misfolding and arthritogenic peptide hypotheses.
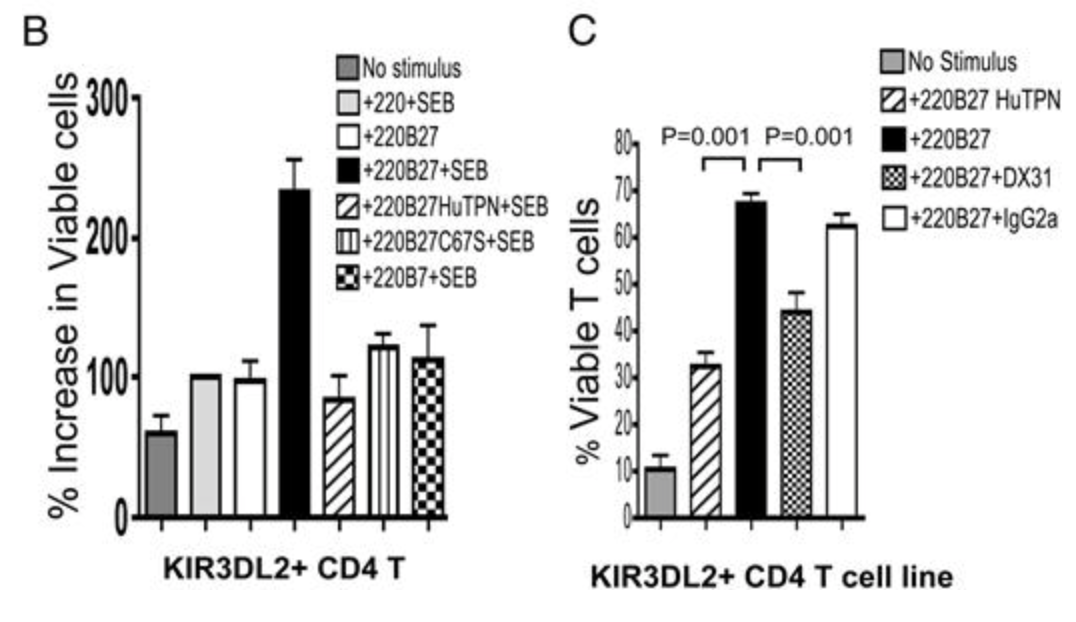
The misfolding hypothesis suggests that the HLA-B27 protein is predisposed to a higher risk of misfolding during translation. When unknown environmental factors trigger misfolding, the result is immune cells that are more inflammatory than other HLA-stimulated immune cells. This misfolding may cause professional antigen-presenting cells (APCs) bearing HLA-B27 proteins to overstimulate helper T cells. In a small trial, Bowness, an immunologist at the University of Oxford, studied this theory. Bowness found these results by taking venous blood samples from 25 patients with AS, six of whom were HLA-B27+ and the remaining 17 were HLA-B27-. Immune cells were isolated by centrifugation and then infected with Staphylococcal enterotoxin B (SEB) bacteria before being stained for surface markers to identify the different cell types and their activation status. Immunoassays were further performed for the levels of IL-17 and IFN-γ produced. The results shown in Table 1 found that KIR3DL2+ CD4+ T cells (immune cells that have been stimulated by HLA-B27 proteins) secreted more IL-17 and had enhanced survival and proliferation rates, strengthening HLA-B27’s association with excessive inflammation.6 This same study also found that KIR3DL2+ CD4+ T cells taken from synovial fluid produced higher levels of TNF-α and IFN-γ compared to corresponding KIR3DL2+ CD4+ T cells taken from peripheral blood. This finding aligns with the typical excessive inflammation found in the joints of AS patients.
The arthritogenic peptide hypothesis was first proposed by immunology researchers and authors Parham and Benjamin in a literature review. The hypothesis states that HLA-B27 presents endogenous self-peptides which appear similar to pathogenic antigens that cytotoxic T cells recognize and bind, generating an immune response.7 This mechanism is generally called molecular mimicry. They tested this theory by using reverse-phase HPLC of the HLA-B27-bound peptide complex after the addition of cytotoxic T cells which showed high binding specificity. To prove the activation and specificity of the T cells, various pathogenic peptides were added, and the results showed high levels of inhibition of the HIV-specific gag peptide but no other peptides.8 Thirty-one years later, a large team of researchers and doctors from the Stanford School of Medicine opened the theory back up by conducting a comprehensive study on patients who were HLA-B27+ and had AS. They took blood samples, isolated the immune cells, and then used single-cell sequencing and structural analysis to visualize the T cell receptor (TCR) and HLA reactions happening. They found that the TCRs bound similarly to the HLA whether it was holding pathogenic or self-antigen. These results presented more evidence to suggest that molecular mimicry may be initiating the excessive inflammatory response. As a next step, the paper’s authors recommend a longitudinal study comparing the T cells of HLA-B27+ individuals from disease onset until death.9
Other Factors
Findings recently published by scientists from the Lanzhou University Second Hospital in China found an interesting difference in the long non-coding RNAs (lncRNA) of mesenchymal stem cells of AS patients when compared with a control group. The donors with AS had more lncRNAs promoting inflammation, specifically TNF-α signaling and NFkB activation, than the healthy donors. The donors with AS also had significantly more lncRNAs which are known activators of osteogenesis, which is believed to be the cause of abnormal bone growth in AS patients.10 Following this study, a research team from New York studied the relationship between AS and bone health. Using a small trial of 30 patients with axial spondyloarthritis, (AS that is most prevalent in the joints), they found that AS disease duration and severity were inversely related to bone mineral density.11
This difference in TNF-α signaling was further explored by scientists from Guangzhou, China, along with the sex differences present in ankylosing spondylitis. Samples of immune cells were extricated from males and females with AS and then run through a database to analyze differentially expressed genes. The results found that males with AS had higher levels of IL-17, but females with AS had a higher count of TNF-α.12 Since IL-17 is one of many cytokines that can activate TNF-α, upregulation of a different cytokine may be causing the AS symptoms in females. These findings indicate that the mechanisms of AS may be different between the sexes, which would explain the sexual dimorphism of the disease prevalence as seen in Figure 1. These findings also suggest that male and female AS patients may benefit from different targeted therapies, although, as of now, the treatment plans for both sexes remain the same.
A paper recently published by Dr. Baeten from the Amsterdam University Medical Center shed some light on the role of IL-17 in the progression of AS. IL-17 inhibitors have long been used to treat the inflammatory symptoms of spondyloarthritis diseases, and so Baeten set up randomized, double-blind clinical trials to test the efficacy of IL-23 inhibitors– a cytokine that activates IL-17. The experimental groups that received IL-23 inhibitors showed no significant symptom resolution or decrease in abnormal bone growth from the control groups. Based on these results, Dr. Baeten suggests that IL-23 may be more important for the initiation phase of AS rather than its chronic phase. This would mean that the IL23/IL17 axis may not be as important to AS progression as was previously assumed, and that IL-23 inhibitors may only be effective if administered in the early stages of disease development.13 However, the study did not specify the sex of the study participants. When considering Li’s findings on sex differences in AS, IL-17 was only elevated in AS males, and so Baeten’s findings on IL-17 may have been confounded by combining males and females in one sample population.
CAR T Cell Therapy
The search for a cure is made more difficult in the disagreement over the cause, and research studying the use of monoclonal antibodies as a cure has since proven ineffective.14 However, recent breakthroughs in CAR T cell therapy initiated a flurry of clinical trials studying its use in the treatment of different diseases. One CAR T cell clinical trial for autoimmune disease patients and two reviews were published in the last year, with more trials in labs across the world in progress. CAR T cells (Chimeric Antigen Receptor T cells) are genetically modified T cells that are similar to monoclonal antibodies in that they have been specialized to target tumor cells in cancer patients, but researchers now believe they can specialize CAR T cells to target and destroy rogue B cells instead.15
A study published in February of 2024 in the New England Journal of Medicine announced its exciting affirmation of this theory. The study took a small sample size of 15 lupus patients who had not responded to other immunosuppressant medications and began CAR T cell therapy. 100% of the patients showed complete lupus remission after one injection, and none have shown relapse of symptoms in the two years since.16 The small sample size was a result of strict inclusion criteria to control for as many confounding variables as possible, including all of their patients having very similar disease severity scores of 13 on the scale called SLEDAI-2K. As the results were significant, follow-up studies with larger sample sizes, involving different patients, were encouraged. UC Davis Health is attempting to recreate these results with a larger sample size, and as of May of 2024 has started a clinical trial to use CAR T cells to treat lupus. Current uses of CAR T cell therapy as a cancer treatment lower B cell counts, causing patients to be more immunocompromised.17,18 If clinical trials for lupus are completed and successful, these CAR T cells may one day be used to target T cell immune diseases, such as ankylosing spondylitis, rather than B cell immune diseases.
The main complication of T-cell targeted CAR T therapy was both described and solved by a group of scientists from London led by Christos Georgiadis and Jane Rasaiyaah. When targeting T cells, scientists commonly develop receptors for the antigens CD3 and CD7, both being specific to T cells. However, when CAR T cells are trained to seek these antigens, they are more likely to kill each other off before reaching their target, a phenomenon that they called “T vs T fratricide.” To generate fratricide-resistant anti-T CAR T cells, Christos and Georgiadis proposed using the CRISPR system to base edit the T cell receptor/CD3 and CD7 antigens from the CAR T cells.19
Discussion/Conclusion
With growing insights into gender differences, immune signaling, and gene regulation, a multifaceted understanding of AS is within reach—provided research efforts continue to bridge science with clinical innovation. Current research shows great promise for the future of patients with ankylosing spondylitis, with CAR T cell research leading the way. However, the hope is that CAR T cell research, as an immunotherapeutic option for AS, does not completely overshadow ongoing efforts to understand the mechanisms behind the disease’s development and progression. Future research should focus on specific characteristics of AS and the HLA-B27 gene to help pinpoint a potential mechanism.
The first area of focus should be longitudinal studies on the patients diagnosed with AS who do not express the HLA-B27 gene. Studies of these individuals can help determine the environmental factors that trigger the development of AS. Immune tissue, blood, synovial fluid, and bone marrow samples from HLA-B27+ and HLA-B27- AS patients can be compared for the classic markers of AS that have already been established. These markers include increased IL-17 and IL-23 in synovial fluid, increased inflammatory lncRNAs in bone marrow, increased HLA misfolding, increased inflammatory cytokines in axial tissue samples, etc.
Another area of possible treatment for AS involves cytokines that are more directly responsible for the disease progression, and not solely the disease initiation. As explained by Dr. Baeten, IL-23 inhibition has been attempted as a therapy but has not been successful. Since the secretion of IL-17 during established AS relies more on IL-1 and IL-18 than IL-23, clinical trials using IL-1 and IL-18 inhibitors for AS patients could be attempted. Conversely, another trial of IL-23 inhibitors could be attempted with a sample of early-onset AS patients to observe if the inhibitors would have more of an effect on that population.
The most promising future for AS remission lies in the field of CAR T cell therapy, depending on the success of attempts to develop CAR T cells against T-cell immune diseases. As discussed in the misfolding hypothesis, KIR3DL2+ CD4+ T cells are overproduced in some HLA-B27+ patients. Theoretically, if CAR T cells specific for KIR3DL2+ CD4+ T cells can be manufactured, it may be able to reverse the effects of HLA-B27 expression. There are so many possibilities in the future for developing treatments for ankylosing spondylitis, as long as research keeps pushing the brink of our gene-based autoimmune knowledge outwards.

About the Author: Grace V Heringer
Grace Heringer is studying Neurobiology, Physiology and Behavior with a minor in Spanish. She grew up here in Davis, and loved the community so much that she decided to study at UC Davis for her undergrad. Now in her fourth year, Grace has been involved in many research projects such as in the Villablanca Lab and Hamada Lab on campus, and interning at KP CREST off campus. When not working on research projects, Grace can be found in the gym coaching volleyball at Davis High School or playing on the Women’s Club Volleyball team. She enjoys the dynamic world of clinical research and hopes to continue working in the field.
Author’s Note
When I signed up for UWP 104f, I knew that I wanted to write my assignments for a good friend of mine who was diagnosed with ankylosing spondylitis. Although it is not an abnormally rare disease, little is known about ankylosing spondylitis besides its main symptoms and association with the HLA-B27 gene. My friend tried to understand all the current research, especially since her options for immunosuppressants are limited and she holds out hope that more treatments will become available soon. I was so excited at this opportunity to summarize the literature for her so she could understand the progress that scientists have made, but also see the same gaps in the literature that I was seeing. Serendipitously, I was also taking a human immunology course this quarter, and lectures from my professor helped me summarize the literature! The professor of the immunology course, Dr. Torres, was heavily involved in immunotherapy and we even briefly touched on ankylosing spondylitis in class. I hope that this review inspires readers to turn their attention towards AS research and the broad horizon of immunotherapy for all autoimmune diseases, including the clinical study happening on our own UC Davis campus.
References
“Spondylitis Association of America - Raising Awareness of Spondyloarthritis.” Spondylitis Association of America - Ankylosing Spondylitis, 13 Nov. 2024, spondylitis.org/.
Navarro-Compán, V., Ermann, J., & Poddubnyy, D. (2022). A glance into the future of diagnosis and treatment of spondyloarthritis. Therapeutic Advances in Musculoskeletal Disease, 14, 1759720X221111611. https://doi.org/10.1177/1759720X221111611
“Ankylosing spondylitis.” (2022, November 16). https://www.hopkinsmedicine.org/health/conditions-and-diseases/ankylosing-spondylitis
Ankylosing Spondylitis: MedlinePlus Genetics. (2022, March 23). https://medlineplus.gov/genetics/condition/ankylosing-spondylitis/. Accessed 15 Feb. 2025.
Gracey, E., Yao, Y., Green, B., Qaiyum, Z., Baglaenko, Y., Lin, A., Anton, A., Ayearst, R., Yip, P., & Inman, R. D. (2016). Sexual dimorphism in the th17 signature of ankylosing spondylitis. Arthritis & Rheumatology, 68(3), 679–689. https://doi.org/10.1002/art.39464
Bowness, P., Ridley, A., Shaw, J., Chan, A. T., Wong-Baeza, I., Fleming, M., Cummings, F., McMichael, A., & Kollnberger, S. (2011). Th17 cells expressing kir3dl2+ and responsive to hla-b27 homodimers are increased in ankylosing spondylitis. The Journal of Immunology, 186(4), 2672–2680. https://doi.org/10.4049/jimmunol.1002653
Bowness, Paul. “HLA-B27.” Annual Review of Immunology, Annual Reviews, 21 Mar. 2015, www.annualreviews.org/doi/10.1146/annurev-immunol-032414-112110
Benjamin, R. J., Madrigal, J. A., & Parham, P. (1991). Peptide binding to empty HLA-B27 molecules of viable human cells. Nature, 351(6321), 74–77. https://doi.org/10.1038/351074a0
Yang, X., Garner, L. I., Zvyagin, I. V., Paley, M. A., Komech, E. A., Jude, K. M., Zhao, X., Fernandes, R. A., Hassman, L. M., Paley, G. L., Savvides, C. S., Brackenridge, S., Quastel, M. N., Chudakov, D. M., Bowness, P., Yokoyama, W. M., McMichael, A. J., Gillespie, G. M., & Garcia, K. C. (2022). Autoimmunity-associated T cell receptors recognize HLA-B27-bound peptides. Nature, 612(7941), 771–777. https://doi.org/10.1038/s41586-022-05501-7
Cen, S., Cai, M., Wang, Y., Lu, X., Chen, Z., Chen, H., Fang, Y., Wu, C., Qiu, S., & Liu, Z. (2022). Aberrant lncRNA–mRNA expression profile and function networks during the adipogenesis of mesenchymal stem cells from patients with ankylosing spondylitis. Frontiers in Genetics, 13, 991875. https://doi.org/10.3389/fgene.2022.991875
Russell, Linda, et al. “Disease Activity and Bone Microarchitectural Phenotype in Patients With Axial Spondyloarthritis.” HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery, July 2024, p. 15563316241268001. DOI.org (Crossref), https://doi.org/10.1177/15563316241268001.
Li S, Chao H, Li Z, Chen S, Zhang J, Hao W, Zhang S, Liu C, Liu H. Sex dimorphism of IL-17-secreting peripheral blood mononuclear cells in ankylosing spondylitis based on bioinformatics analysis and machine learning. BMC Musculoskelet Disord. 2024 Jun 24;25(1):490. doi: 10.1186/s12891-024-07589-6. PMID: 38914997; PMCID: PMC11194900.
Baeten, Dominique, and Iannis E. Adamopoulos. “IL-23 inhibition in ankylosing spondylitis: Where did it go wrong?” Frontiers in Immunology, vol. 11, 18 Feb. 2021, https://doi.org/10.3389/fimmu.2020.623874
Schett, G., Mackensen, A., & Mougiakakos, D. (2023). CAR T-cell therapy in autoimmune diseases. The Lancet, 402(10416), 2034–2044. https://doi.org/10.1016/S0140-6736(23)01126-1
Connolly, Liam. “A Breakthrough for Lupus Treatment? Study Explores Car T-Cell Therapy for Autoimmune Disease.” UCDavisHealthNews, UC Davis Health, 22 May 2024, health.ucdavis.edu/news/headlines/a-breakthrough-for-lupus-treatment-study-explores-car-t-cell-therapy-for-autoimmune-disease/2024/05.
Müller, F., Taubmann, J., Bucci, L., Wilhelm, A., Bergmann, C., Völkl, S., Aigner, M., Rothe, T., Minopoulou, I., Tur, C., Knitza, J., Kharboutli, S., Kretschmann, S., Vasova, I., Spoerl, S., Reimann, H., Munoz, L., Gerlach, R. G., Schäfer, S., … Schett, G. (2024). Cd19 car t-cell therapy in autoimmune disease—A case series with follow-up. New England Journal of Medicine, 390(8), 687–700. https://doi.org/10.1056/NEJMoa2308917
Chen, Gregory M., et al. “B Cell Targeting in CAR T Cell Therapy: Side Effect or Driver of CAR T Cell Function?” Science Translational Medicine, vol. 14, no. 650, June 2022, p. eabn3353. PubMed Central, https://doi.org/10.1126/scitranslmed.abn3353.
Mullard, Asher. “CAR T Cell Therapies Raise Hopes — and Questions — for Lupus and Autoimmune Disease.” Nature Reviews Drug Discovery, vol. 22, no. 11, Oct. 2023, pp. 859–61. www.nature.com, https://doi.org/10.1038/d41573-023-00166-x
Georgiadis, Christos, et al. “Base-Edited CAR T Cells for Combinational Therapy against T Cell Malignancies.” Leukemia, vol. 35, no. 12, 2021, pp. 3466–81. PubMed Central, https://doi.org/10.1038/s41375-021-01282-6.