
GLP-1 Receptor Agonists' Impact on Cardiovascular Disease Outcomes in Patients with Type 2 Diabetes
Abstract
Objective: Identify how GLP-1 receptor agonists affect cardiovascular disease outcomes in type 2 diabetics. Methods: Databases such as Pubmed, Scopus and ScienceDirect were accessed via the UC Davis library to obtain articles. Articles that were randomized controlled trials within a 5 year span were prioritized. The criteria for selecting articles were those concerned with type 2 diabetic patients that are taking GLP-1 receptor agonists to assess cardiovascular disease outcomes. Results: The articles showed consistent trends of weight reduction, lowered HbA1c and improved cardiovascular disease outcomes in type 2 diabetic patients compared to placebo groups. Factors such as chemical byproducts, physical limitations and cardiovascular events were improved with the administration of this medication. Conclusion: GLP-1 receptor agonists improve cardiovascular disease outcomes in type 2 diabetic patients. The articles that were sourced prioritized the use of a specific GLP-1 receptor agonist (Semaglutide), which does not reflect all GLP-1 receptor agonists having similar effects and outcomes. No long-term study follow ups have been recorded, which means only short-term effects are recorded.
Keywords: GLP-1 receptor agonist, cardiovascular disease, type 2 diabetes, obesity
Introduction
It's no surprise that a drug that effectively promotes weight loss is turning heads in today’s media. The most popular medication that is being utilized for this effect is called Ozempic or Semaglutide, which falls into the category of glucagon-like peptide-1 (GLP-1) receptor agonists. Due to the popularity of this medication it is important to see how it impacts certain aspects of type 2 diabetic comorbidities. This medication is tailored to both obese and type 2 diabetic individuals to improve their conditions. Type 2 diabetes typically has comorbidities with other diseases such as hyperlipidemia, cardiovascular disease/heart failure and hypertension, which may contribute to obesity. It is well known that weight reduction is a common outcome with this semaglutide, but it has been shown that some comorbidities that are tied in with type 2 diabetes are also improved. Consequently, cardiovascular disease can be fatal especially when compounded with the background effects of type 2 diabetes. Therefore this review of literature focuses on how cardiovascular disease improves in type 2 diabetic patients taking GLP-1 receptor agonists [1].
Endocrine Glands of the Pancreas
Understanding how the pancreas functions can give better insight both on how diabetes works and how it impacts cardiovascular disease. The pancreas is composed of both endocrine and exocrine glands, where 98% of the gland is exocrine and 2% is endocrine. The exocrine glands are the major digestive organ in the gastrointestinal system, while the endocrine glands release hormones based on blood glucose levels. Within the endocrine glands are the islets of Langerhans which house alpha, beta and delta cells. The alpha cells will secrete glucagon when blood glucose levels are low, which communicates to the liver to make new glucose [2]. Beta cells secrete insulin and urocortin 3 (a signaling molecule within the islets). Insulin is secreted in response to food stimuli so that glucose can be brought into cells to be metabolized and stored as glycogen for future use. Urocortin 3 is secreted by both alpha and beta cells in humans. Additionally, it is abundantly expressed in beta cells and is co-secreted with insulin to promote somatostatin secretion from delta cells as a negative feedback mechanism to inhibit insulin and glucagon [3].
Type 2 Diabetes and its physiology
Obesity can be defined as having a BMI of 30 kg/m2 to upwards to over 40 kg/m2 and is increasing in populations rapidly [4]. In the United States, projections indicate that by 2030, 48.9% of adults will be classified as obese, with 24.2% experiencing severe obesity (BMI ≥35). This burden is expected to increase susceptibility for severe obesity within certain populations, including non-Hispanic Black adults, women, and individuals with low income[5]. Obesity contributes to the mechanism of type 2 diabetes, which makes insulin not sensitive to its receptors. Moreover, cardiovascular disease with type 2 diabetes cases are expected to rise rapidly for the next 30 years, making this a topic of research that should be investigated. Individuals with type 2 diabetes face a sixfold higher risk of developing cardiovascular disease compared to their non-diabetic counterparts [7].
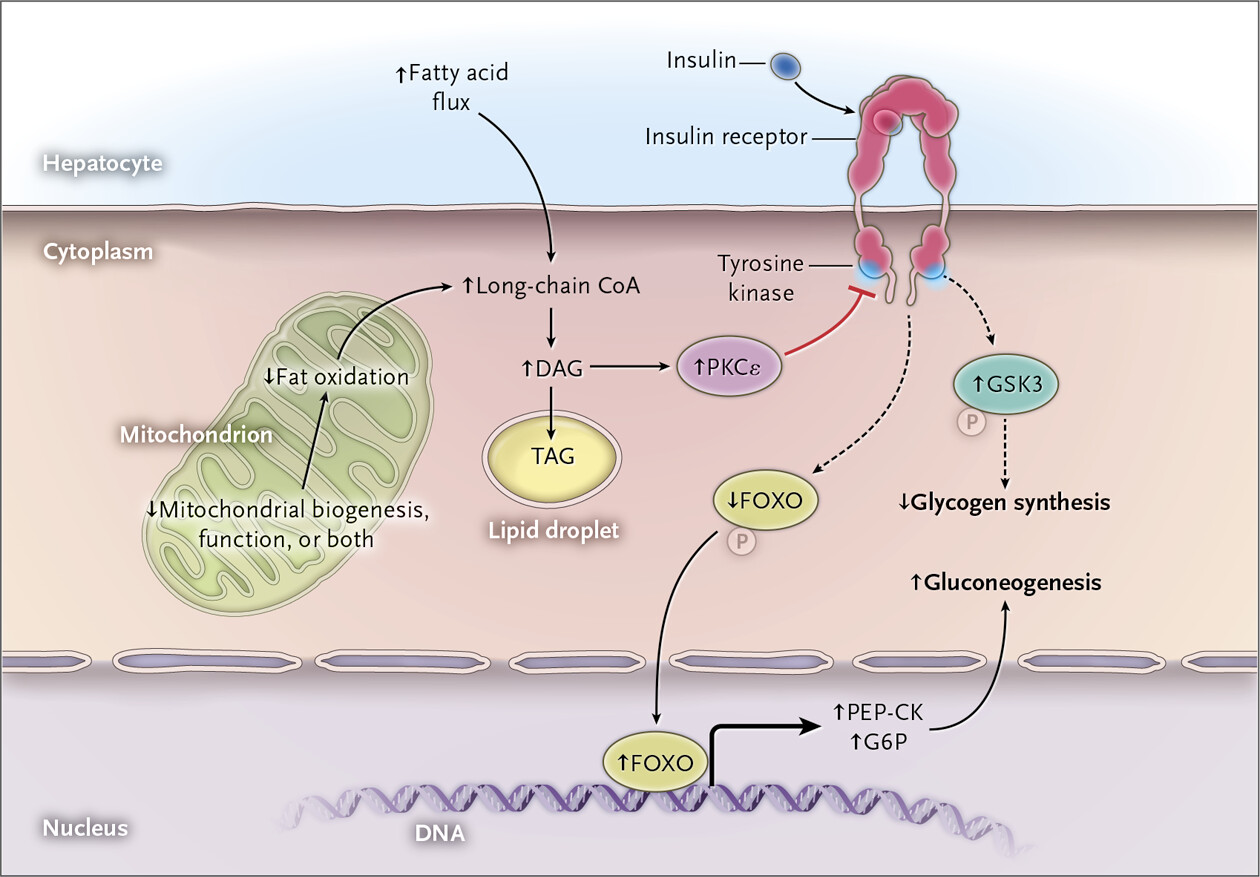
Classified as a metabolic disorder, diabetes mellitus results in elevated blood glucose levels through different physiological mechanisms. Type 2 diabetes is the most prevalent form, comprising 90–95% of cases, in contrast to type 1 diabetes. The onset of type 2 diabetes typically occurs after the age of 30 and between the ages of 50 and 60, where it will then develop gradually. These individuals will have hyperglycemia due to a multitude of factors such as impaired insulin secretion and impaired carbohydrate metabolism. Among these factors, insulin resistance plays a central role and for metabolic syndrome, which includes symptoms such as obesity, hypertension, decreased blood high-density lipoprotein-cholesterol, fasting hyperglycemia and increased blood triglycerides in the blood. Additionally, one of the major consequences of developing metabolic syndrome is cardiovascular disease, more specifically atherosclerosis [8]. Excess fat within muscles can yield insulin resistance by interfering with insulin signaling. Therefore, there will be an increase of fatty acids that do not get oxidized or broken down fast enough resulting in the activation of a protein called PKC (protein kinase C theta). PKC will act to oppose the intended functions of the insulin receptor by phosphorylating specific substrates on the receptor, reducing the amount of glucose entering the muscle and decreasing glycogen (stored glucose) synthesis. In the liver, insulin resistance occurs similar to resistance in muscle tissue in which an excess amount of unoxidized fatty acids activate a protein called PKC, which will interfere with the insulin receptors in the liver. This protein will decrease glycogen synthesis and activate genes for gluconeogenesis (a mechanism in the body in which glucose is made by substrates to increase blood glucose in hypoglycemic situations), ultimately increasing the severity of high blood glucose levels. Excess levels of circulating fat will also be infiltrated by macrophages, which will break down fat products and activate gluconeogenesis in the liver contributing to high blood glucose levels [9].

GLP-1 Receptor Agonist Physiology
GLP-1 receptor agonists, made by L cells in the ileum and the early colon, are a typical treatment for managing type 2 diabetes. GLP-1 receptor agonists act to mimic incretins (gastrointestinal hormones that promote insulin secretion), which aid with the release of insulin and suppression of glucagon. They are also located in the central nervous system and in the alpha cells in the pancreas. The presence of food will stimulate the L cells and release this incretin. GLP-1 receptor agonist molecules bind to the same receptors that GLP-1’s do and are able to last longer due to having a different chemical structure that does not degrade as easily. These mimic elicit responses such as weight loss, delayed gastric emptying, and lowered blood sugar [10]. Although GLP-1 receptor agonists are well known for their weight loss benefits and blood sugar-lowering effects, their impact on cardiovascular disease outcomes should also be evaluated to determine whether they improve not only type 2 diabetes but also cardiovascular health.
Methods
The patient inclusion criteria for these articles were presence of obesity (BMI >30), type 2 diabetes, and current usage of GLP-1 receptor agonists (semaglutide being the most popular). Cardiovascular disease outcomes should be evaluated after taking this medication to see if there was any improvement. The articles chosen were limited to the last 5 years due to the rapidly evolving field of medicine. The exclusion criteria for the articles are patients who have non-cardiovascular disease comorbidities with type 2 diabetes, and type 1 diabetic patients. Medications that are also being taken in tandem with the GLP-1 receptor agonist will also be excluded.
The UC Davis library was used to access specific databases such as Scopus, ScienceDirect and Pubmed. Due to the physiological nature of the research question, Pubmed was optimized. ScienceDirect is a helpful database to obtain articles that were not included in pubmed and Scopus. Articles were sourced using advanced search options on these databases with the use of boolean operators. While creating an annotated bibliography for the research question, a matrix was used to find similarities and common themes of the articles. It also assisted with the process of excluding non-pertinent articles. After utilizing a matrix, Illicit AI was used to compare and source articles that did not emerge directly in the UC Davis library databases.
Critical appraisal tools from CASP were utilized for each article to show strengths and weaknesses of each article. Each assessment of the article involved a checklist of criteria in a PDF, which was provided by CASP. Another critical appraisal resource by Joanna Brigss was used to assess articles. Research articles that were randomized controlled trials and meta-analysis’ were chosen for the foreground information to show direct effects of the medication on cardiovascular disease. Literature reviews and medical physiology textbooks were used for background information to build a foundation and give general knowledge on these topics. All articles that were chosen were peer reviewed to ensure credibility. Articles that showed similar tests or repeated trials were excluded, with the exception of the meta-analysis utilizing similar data between articles. Although these articles share similar themes and outcomes, different cardiovascular aspects were encouraged for analysis to create a diverse approach to assessing cardiovascular disease.
Results
Improvement of Cardiovascular Disease Symptoms and Physical Capabilities
Kosiborod, et al. (2024) conducted a randomized controlled trial that evaluated the cardiovascular outcomes of semaglutide in patients with type 2 diabetes and a form of heart failure [11]. The trial size consisted of 616 participants randomized at a 1:1 ratio to either receive semaglutide or a placebo. The drug and placebo were introduced to patients who had heart failure with a preserved ejection fraction (showing signs and symptoms of heart failure with diastolic abnormalities on EKG with preserved ejection fraction) of 45%, a BMI of 30 or more, an HbA1c of no more than 10% and type 2 diabetes for at least 90 days [12]. The methodology for this study involved patients who were randomly assigned to receive a once weekly 2.4mg semaglutide or a placebo on a 1:1 ratio for 52 weeks. Semaglutide administration started at 0.25mg for 4 weeks, which then would gradually increase every 4 weeks until the dose reached 2.4mg at week 16. The primary endpoints dealt with a change in the Kansas City cardiomyopathy questionnaire clinical score (KCCQ-CSS). This scoring method ranges from 0-100, where high scores represent fewer symptoms, physical limitations and changes in body weight. The secondary endpoints assessed a change in 6 minute walk distance, c-reactive protein level and it also reassessed the KCCQ-CSS. The double blind, randomized, placebo controlled trials were done in 16 countries in Asia, Europe, North and South America. The KCCQ-CCS scored 13.7 points with semaglutide, while the placebo group scored 6.4. The average change in body weight for patients taking semaglutide was -9.8%, while it was -3.4% with the placebo group. The secondary endpoints favored semaglutide. The 6 minute walk distance showed a 14.3 m difference between the semaglutide group and the placebo, while the treatment ratio for change in CRP was 0.67. The discussion mentions the benefits of this medication, such as lowering CRP levels and reducing risk of heart failure. It also mentions the typical treatment plans that type 2 diabetics have and how Kosiborod, et al. (2024) was able to narrow down which patients were eligible for trials [11]. It was concluded that semaglutide’s effect on cardiovascular disease symptoms and limitations on the patients physical capabilities were reduced.
Meta-Analysis of Risk of Cardiovascular Events (Stroke and Myocardial Infarction)
Qin, et al. (2022) conducted a meta-analysis with the purpose of evaluating the risk of cardiovascular events (stroke and myocardial infarction) of type 2 diabetics that use GLP-1 receptor agonists [13]. The articles that were sourced consisted of double blind randomized controlled trials. The population included type 2 diabetic patients that were randomized to take either a placebo or GLP-1 receptor agonist. Patients that have type 2 diabetes with or without cardiovascular disease while using the GLP-1 receptor agonist or placebo were also included within this meta-analysis. Cardiovascular outcomes of interest included death from cardiovascular cause, fatal or non-fatal stroke and fatal or non-fatal myocardial infarction. Overall the analysis consisted of 6 double blind RCT which included 52,821 diabetic patients. The results showed that the GLP-1 receptor agonist decreased the risk of death from cardiovascular disease. The risk of stroke results were reduced from GLP-1 receptor agonists compared to the placebo, while the medication did not have a notable influence on fatal vs non-fatal myocardial infarction compared to the placebo group. Overall Qin, et al. (2022) concluded that this medication has the potential to decrease the likelihood of death from cardiovascular causes and fatal or nonfatal stroke compared to the placebo [13].
Vascular Regenerative Progenitor Cells
A randomized controlled trial done by Park, et al. (2024) showed the effects of GLP-1 receptor agonists and SGLT-2 inhibitors on vascular regenerative progenitor cells in patients with type 2 diabetes. There were a total of 92 patients with type 2 diabetes: 20 individuals taking the GLP-1 receptor agonist, 42 individuals taking the SGLT-2 inhibitor and 30 individuals taking neither. The results showed that the individuals taking the GLP-1 receptor agonist had more vascular regenerative cells in contrast to the other two groups. The other two groups had similar levels of vascular regenerative cells present. Pro-inflammatory monocyte precursors were also measured, showing the opposite trend to the vascular regenerative cells. The GLP-1 receptor agonist group had the lowest level of these precursors, while the SGLT-2 inhibitor and “neither” groups had higher and similar concentrations [14].
Oral Administration Opposed to Subcutaneous Injection
Husain et al. (2019) ran a randomized controlled trial on whether a once-daily oral administration of semaglutide had a noninferior cardiovascular risk to patients who are at high risk for cardiovascular disease and type 2 diabetic. 3183 patients were randomized on a 1:1 ratio for either a placebo or oral semaglutide medication. The trials were conducted as event-driven, randomized, double blind and placebo-controlled. This trial ran for 15.9 months and showed that major adverse cardiovascular events for the group who took semaglutide was 61/1592 or 3.8%, while the placebo group had 76/1592 or 4.8%. This concludes that the cardiovascular risk in type 2 diabetics when taking oral semaglutide was not inferior to the placebo [15].
Conclusion
The articles that were presented showed a detailed understanding on how GLP-1 receptor agonists worked in relation to cardiovascular disease. The literature review written by Moore, et al. (2023) focused on the effect of specific medications in the treatment of obese and type 2 diabetic patients, with a huge emphasis on GLP-1 receptor agonists, which gives a complete foundation to the research question [16]. Weight loss as the main effect of the GLP-1 receptor agonist was consistent with articles written by Kosiborod [11]; Qin [13] and Husain [15]. A decrease in HbA1c or lowered glucose was also a known effect that occurs when taking this medication, which was mentioned in the articles written by Husain [15] and Qin [13]. The literature by Moore, et. al (2023) shows that semaglutide groups were able to reduce a patient’s weight from between a -14.9% reduction to a -16% reduction, while the placebos had a lower weight reduction from -2.4% to 6.2% [16].
For the resources that were chosen, different GLP-1 receptor agonists were utilized. Although there were different variations of the medication, a common theme of Semaglutide administration aside from other analogs was the most popular and effective in relation to cardiovascular disease outcomes [11, 13, 14, 15, & 16].
A common trend among the articles in this literature review is the demonstrated improvement in cardiovascular disease outcomes. However, each study approached this improvement from a unique perspective, interpreting cardiovascular benefits through different measures. These included outcomes in physical limitations, different routes of administration for the same medication (Semaglutide), occurrences of specific cardiovascular events such as stroke and heart attack, and the presence of regenerative cells that aid in cardiovascular disease recovery. Limitations on the subject’s physical capabilities were reduced in the literature by Kosiborod, et al. (2024), showing an improvement with the semaglutide group opposed to the placebo group [11]. Improvement was also shown by the KCCQ-CSS scoring method, with the semaglutide group scoring higher than the placebo group, demonstrating fewer symptoms, and decreasing weight in addition to improved physical capabilities. A misrepresentation in population due to racial imbalances may affect results. It was noted that the percentage of Black patients that were from the United States was 26%, which is a greater percent compared to the national population that was reported to have heart failure and preserved ejection fractions, which also aligns with the trends that non-hispanic Black adults are more susceptible to obesity [5]. The non-White participants in these trials were low, which had the potential to affect the generalization of the data. This study was also limited due to not having any follow ups post one year after the trials [11]. The meta-analysis that was chosen for this literature review demonstrated that the administration of semaglutide in obese type 2 diabetic subjects decreased the occurrence of death from stroke, while death from myocardial infarction did not have much of a difference compared to the placebo group [11]. It should be noted that only published trials were included for this meta-analysis, which may not show the full extent of the effect of GLP-1 receptor agonists and occurrences of stroke and myocardial infarction [13]. Administration of semaglutide in an oral form opposed to injection showed no big differences with cardiovascular risk groups. Although this is a different route of administration, the desired effect is still consistent with the subcutaneous medications, showing consistency in improved cardiovascular disease outcomes [15]. The occurrence of vascular regenerative progenitor cells was increased in subjects taking the GLP-1 receptor agonist compared to the other groups (placebo and SGLT-1 inhibitor groups). Having high levels of vascular regenerative cells establishes a foundation for more proliferative hematopoietic (dividing blood cells) and endothelial colony-forming cells (cells located within the endothelium of blood vessels) to be present. It would also be beneficial in recovery of ischemic (narrowing) vessels by promoting more reparative cells. Another great addition from this research showed a decrease of pro-inflammatory monocyte precursors in the GLP-1 receptor agonist group highlighting a decrease in future inflammatory events. These trends should be considered when trying to reduce major cardiovascular events (MACE). An important perspective to note with this literature is that the endpoints of the initial study (ORIGINS-RCE Cardiolink-13) were not designed to interpret the endpoints of this subanalysis, which may limit if these findings are valid [14]. Additionally, the literature by Husain et al. (2019) showed that even though there was a different route of administration, the desired effect is still consistent with the subcutaneous medications, showing consistency with improved cardiovascular disease outcomes [15].
A majority of the articles selected were funded by a pharmaceutical company called Novo Nordisk. Although this company is funding the research, outsider perspectives can form opinions on whether or not promoting this medication as a pharmaceutical company is ethical [11, 14, & 15].

About the Author: Dillon Schmidt
Dillon graduated from UC Davis in 2025 with a major in Neurobiology, Physiology, and Behavior.
Author's Note
I was briefly introduced to the concept of diabetes in my introductory physiology classes, which left me curious to learn more. Fortunately for me, UC Davis offers a course for diabetes physiology and its management. After taking this course, my diabetes knowledge has increased exponentially and has since then directed my physiology interests into endocrinology and hormone disorders.
References
Singh G, Krauthamer M, Bjalme-Evans M. 2022. Wegovy (semaglutide): a new weight loss drug for chronic weight management. J Investig Med [Internet]. 70(1):5–13. https://doi.org/10.1136/jim-2021-001952
Masharani U, German MS. 2017. Pancreatic hormones and diabetes mellitus. In: Gardner DG, Shoback D, editors. Greenspan's Basic & Clinical Endocrinology, 10e. New York (NY): McGraw-Hill Education. https://accessmedicine.mhmedical.com/content.aspx?bookid=2178§ionid=16625195
Van der Meulen T, Donaldson CJ, Cáceres E, Hunter AE, Cowing-Zitron C, Pound LD, Adams MW, Zembrzycki A, Grove KL, Huising MO. 2015. Urocortin3 mediates somatostatin-dependent negative feedback control of insulin secretion. Nat Med. 21(7):769–776. https://doi.org/10.1038/nm.3872
Zierle-Ghosh A, Jan A. 2023. Physiology, Body Mass Index. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK560891/
Ward ZJ, Bleich SN, Cradock AL, Barrett JL, Giles CM, Flax C, Long MW, Gortmaker SL. 2019. Projected U.S. State-Level Prevalence of Adult Obesity and Severe Obesity. N Engl J Med. 381(25):2440–2450. https://doi.org/10.1056/NEJMsa1909301
Nauck MA, Quast DR, Wefers J, Meier JJ. 2021. GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-the-art. Mol Metab. 46:101102. https://doi.org/10.1016/j.molmet.2020.101102
Mechanick JI, Farkouh E. 2022. Diabetes and cardiovascular disease. In: Fuster V, Narula J, Vaishnava P, Leon MB, Callans DJ, Rumsfeld JS, Poppas A, editors. Fuster and Hurst's The Heart, 15e. New York (NY): McGraw-Hill Education.
Hall JE, Guyton AC. 2011. Guyton and Hall textbook of medical physiology. 12th ed. Philadelphia (PA): Saunders/Elsevier.
Shulman GI. 2014. Ectopic fat in insulin resistance, dyslipidemia, and cardiometabolic disease. N Engl J Med. 371(12):1131–1141. https://doi.org/10.1056/NEJMra1011035
Zhao X, Wang M, Wen Z, Lu Z, Cui L, Fu C, Xue H, Liu Y, Zhang Y. 2021. GLP-1 receptor agonists: beyond their pancreatic effects. Front Endocrinol (Lausanne) [Internet]. 12:721135. https://doi.org/10.3389/fendo.2021.721135
Kosiborod MN, Petrie MC, Borlaug BA, Butler J, Davies MJ, Hovingh GK, Kitzman DW, Møller DV, Treppendahl MB, Verma S, et al. 2024. Semaglutide in patients with obesity-related heart failure and type 2 diabetes. N Engl J Med. 390(15):1394–1407. https://doi.org/10.1056/NEJMoa2313917
Shah KS, Xu H, Matsouaka RA, Bhatt DL, Heidenreich PA, Hernandez AF, Devore AD, Yancy CW, Fonarow GC. 2017. Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes. J Am Coll Cardiol. 70(20):2476–2486. https://doi.org/10.1016/j.jacc.2017.08.074
Qin J, Song L. 2022. Glucagon-like peptide-1 (GLP-1) receptor agonists and cardiovascular events in patients with type 2 diabetes mellitus: a meta-analysis of double-blind, randomized, placebo-controlled clinical trials. BMC Endocr Disord [Internet]. 22(1):125. https://doi.org/10.1186/s12902-022-01036-0
Park B, Krishnaraj A, Teoh H, Bakbak E, Dennis F, Quan A, Hess DA, Verma S. 2024. GLP-1RA therapy increases circulating vascular regenerative cell content in people living with type 2 diabetes. Am J Physiol Heart Circ Physiol. 327(2):H370–H376. https://doi.org/10.1152/ajpheart.00257.2024
Husain M, Birkenfeld AL, Donsmark M, Dungan K, Eliaschewitz FG, Franco DR, Jeppesen OK, Lingvay I, Mosenzon O, Pedersen SD, et al. 2019. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 381(9):841–851. https://doi.org/10.1056/NEJMoa1901118
Moore PW, Malone K, VanValkenburg D, Rando LL, Williams BC, Matejowsky HG, Ahmadzadeh S, Shekoohi S, Cornett EM, Kaye AD. 2023. GLP-1 agonists for weight loss: pharmacology and clinical implications. Adv Ther. 40(3):723–742. https://doi.org/10.1007/s12325-022-02394-w